When your kidneys fail, dialysis isn't just a medical procedure-it becomes part of your daily life. For many people, doing dialysis at home is the best way to keep living like yourself. Two main ways to do this are Continuous Ambulatory Peritoneal Dialysis (CAPD) and Automated Peritoneal Dialysis (APD). Both use your abdominal lining as a natural filter, but they work in completely different ways. Choosing between them isn't about which is better overall-it's about which fits your body, your schedule, and your home.
How CAPD Works: Manual, Every Day
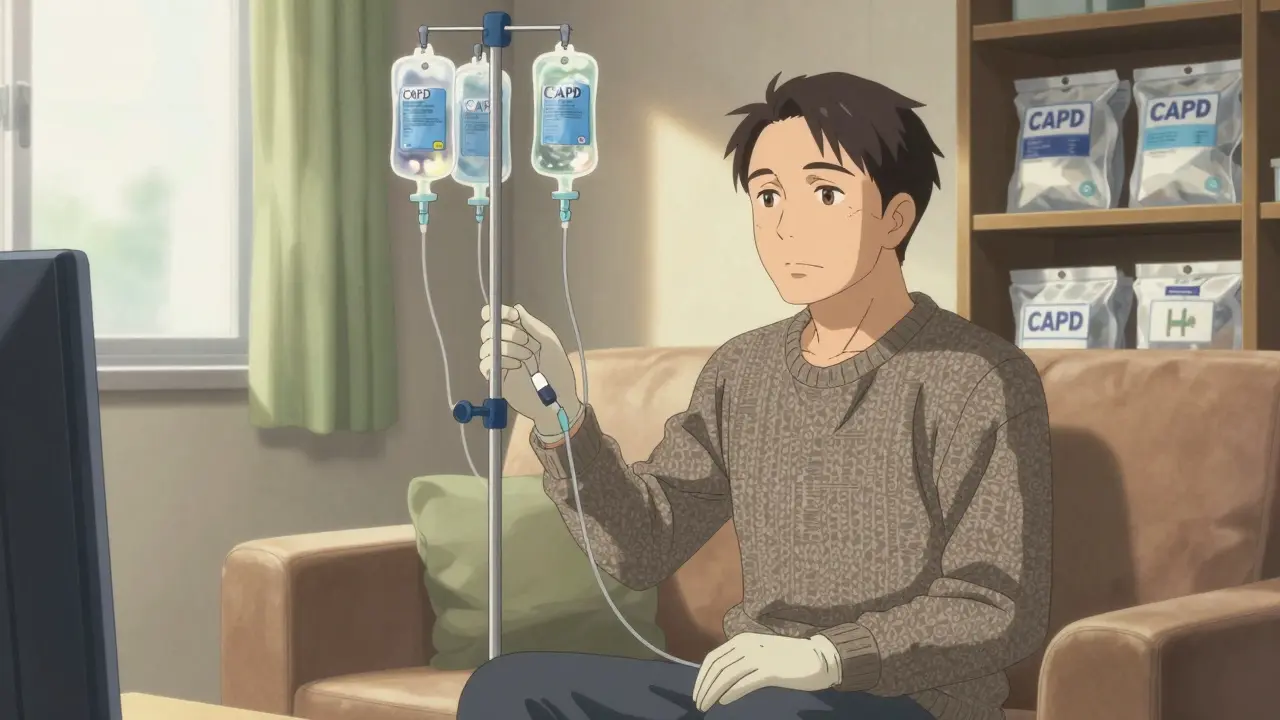
CAPD doesn’t need a machine. You do it yourself, four to five times a day, using gravity. You connect a bag of dialysis fluid to a catheter in your belly, let it sit for about four to six hours, then drain it out. Each exchange takes 30 to 40 minutes. You can do it while sitting, watching TV, or even at work. No electricity. No setup. Just clean hands, a clean space, and the right technique.
That’s the trade-off. You carry around 4 to 6 pounds of fluid bags every day. You have to plan your day around exchanges. If you’re a teacher, a delivery driver, or someone who travels often, this flexibility is a huge plus. You can do an exchange during a lunch break, a commute, or even on a plane. But if you have arthritis, shaky hands, or trouble bending over, it can become a daily struggle. About 34% of people who switch off CAPD do so because they can’t manage the manual steps safely-and that often leads to infection.
How APD Works: Automatic, While You Sleep
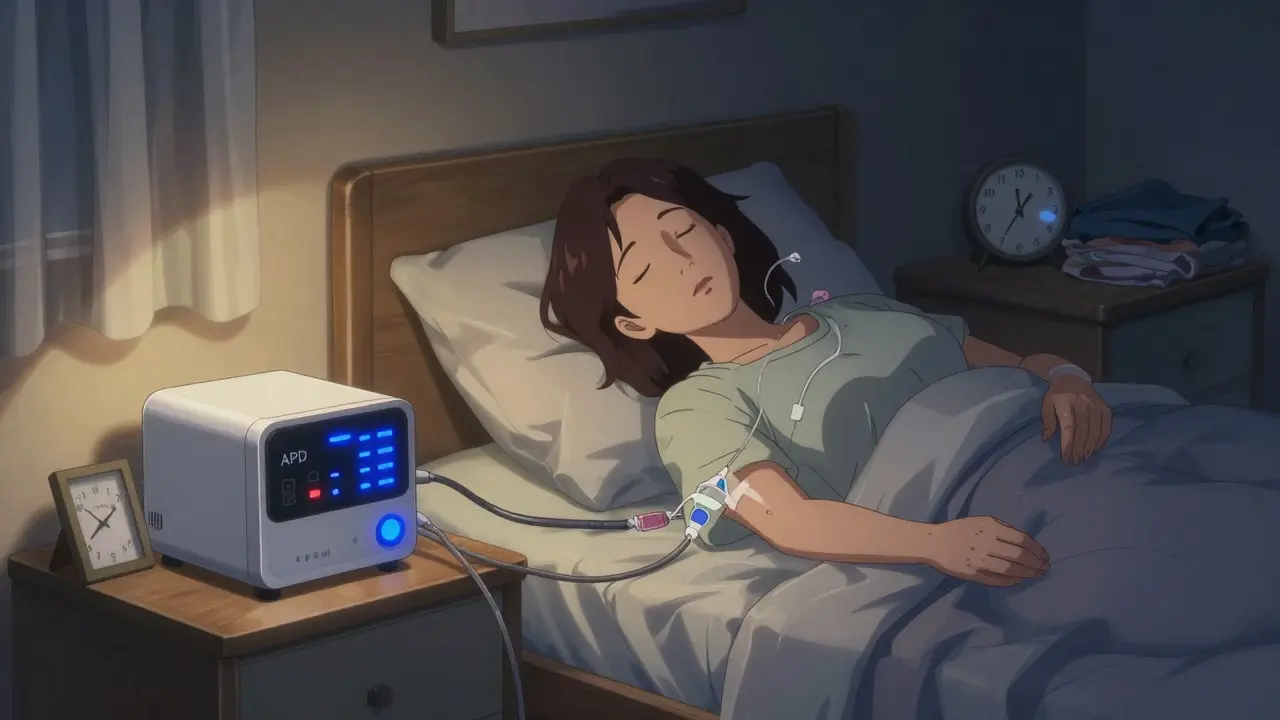
APD uses a machine-a cycler-that does the work while you sleep. You hook up to it before bed, and it fills your belly with fluid, lets it sit, then drains it out automatically over 8 to 10 hours. You wake up with clean blood, no interruptions. Modern cyclers like the Baxter Amia or Fresenius Sleep-Safe are quiet, about the noise level of a library. They weigh 15 to 25 pounds and need a small space and an electrical outlet.
This is why APD is popular among working adults. One ER nurse in her 40s told us she works 12-hour shifts without missing a beat. The machine handles everything. No daytime exchanges. No carrying bags. But there’s a catch. If the machine breaks down-about 12% of users face this each year-you need to switch to manual exchanges right away. And if your power goes out? You’re stuck. Also, some people can’t sleep with the machine running, even if it’s quiet. One in five APD users stop because the noise or the setup feels too intrusive.
Which One Is Safer?
Safety isn’t just about infection-it’s about consistency. CAPD has a higher risk of peritonitis (abdominal infection) because every exchange is manual. Each time you connect a bag, you’re opening a pathway to bacteria. The average rate is 0.68 infections per person per year. APD, with its closed system and automated connections, brings that down to 0.52. That might sound small, but over time, it means fewer hospital trips and better long-term outcomes.
Fluid control matters too. APD removes fluid more steadily because it’s happening all night. This leads to 22% fewer cases of dangerous fluid overload, which can cause high blood pressure or heart strain. CAPD works well too, but it’s less consistent. If you miss an exchange or do one too slowly, fluid builds up. That’s why APD users have lower rates of hypertension emergencies and need fewer blood pressure meds.
Cost and Accessibility
In the U.S., Medicare covers 80% of both CAPD and APD costs. But out-of-pocket expenses differ. CAPD supplies cost $50 to $75 a month. APD runs $75 to $100 because you’re renting the cycler. Some insurance plans cover the rental, but not all. In rural areas, getting a cycler delivered or serviced can take weeks. CAPD is easier to support remotely-nurses can check in by phone. APD needs tech support for machine issues, and not every clinic offers 24/7 help.
There’s also the hidden cost of space. CAPD needs storage for bags. APD needs a dedicated corner with an outlet, room for the machine, and space to store tubing and supplies. If you live in a small apartment or share a room, APD might not be practical. Studies show 23% of home dialysis candidates need home modifications before starting-and that’s harder to arrange if you’re low-income or renting.
Who Benefits Most from Each?
There’s no one-size-fits-all answer. But patterns are clear.
If you’re over 65, have trouble with fine motor skills, or live in a place without reliable power, CAPD is often the better fit. It’s simpler. No tech to break. No setup to learn. One nephrologist told us, “CAPD is the gold standard for patients over 75.”
If you’re under 65, work full-time, care for kids, or want to sleep through your treatment, APD wins. It gives you back your days. And with newer cyclers that monitor your fluid levels automatically and adjust treatment remotely, it’s getting smarter. One 2022 study showed APD users slept 3.2 hours more per night than CAPD users. That’s not just comfort-it’s health.
But here’s the thing: you don’t have to pick forever. Some people start with CAPD and switch to APD later. Others try APD, find the machine too much, and go back to manual exchanges. Your needs change. Your body changes. Your life changes. That’s why regular check-ins with your care team matter more than the machine you use.
What You Need to Know Before Starting
Training is serious. CAPD takes 10 to 14 days of daily practice. You learn sterile technique, how to spot infection signs, and how to handle emergencies. APD training is longer-14 to 21 days-because you’re learning a machine. You need to know how to reset it, clear air bubbles, and what to do if the alarm goes off at 2 a.m.
Both need a clean, dry space. No pets. No clutter. No sharing a bathroom with someone who’s sick. You’ll need storage for supplies-about a 4x4 foot area. And you’ll need someone nearby who can help if you get sick. That’s why Medicare now allows family members to be trained as care partners. It’s not optional anymore-it’s essential.
Remote monitoring is changing the game. APD systems today can send data to your nurse every day. If your fluid balance is off, they can adjust your treatment before you even feel sick. CAPD doesn’t have this yet. That’s why APD is growing faster. By 2030, it’s expected to be the most common home dialysis method.
Real People, Real Choices
One 58-year-old teacher in Ohio does CAPD during his planning periods. He keeps bags in his closet. “I’ve done it for seven years. I never miss a day. I don’t need a machine-I need freedom.”
A 42-year-old nurse in Texas uses APD. “I work nights. The cycler runs while I sleep. I’ve had three breakdowns. Each time, I had to call for help. But I still choose it. I get to live my life.”
Both are right. Neither is better. It’s about what fits your life right now.
What’s Next?
The future of dialysis is moving toward smarter, quieter, more connected systems. New cyclers can now adjust treatment based on your weight and blood pressure. Some are even being tested with smartphone apps. By 2025, the first phone-connected cycler could be approved. That means fewer errors, fewer hospital visits, and more control for you.
But the core truth hasn’t changed: home dialysis gives you back your life. Whether you choose CAPD or APD, you’re choosing independence. You’re choosing to wake up, go to work, hug your grandkids, or take a trip-without being tied to a clinic three times a week.
The best choice isn’t the one with the fanciest tech. It’s the one you can stick with.
Can I switch from CAPD to APD later?
Yes, many people switch. If you start with CAPD and find the manual exchanges too tiring, or if your health changes, switching to APD is common. Your care team will guide you through training and equipment setup. The catheter stays in place, so no extra surgery is needed. The same goes for switching from APD to CAPD-if the machine becomes too much, going back to manual exchanges is possible.
Is one method better for older adults?
For most people over 75, CAPD is often recommended because it doesn’t require operating a machine. Cognitive decline, shaky hands, or arthritis can make APD setup difficult. But if an older person has strong support at home-like a spouse or caregiver who can handle the cycler-APD can still be a great option. The key isn’t age-it’s ability, support, and personal preference.
Do I need a caregiver to do either type of dialysis?
It’s strongly recommended, especially for APD. While CAPD can be done alone, having someone nearby to help during infections or emergencies improves safety. For APD, caregivers can assist with setup, troubleshooting, or nighttime alarms. Medicare now allows family members to be trained as official care partners, which helps reduce hospitalizations and makes home dialysis more sustainable.
What if my power goes out while using APD?
If your power goes out, you must switch to manual exchanges immediately. Your care team will train you on how to do this using gravity-based methods-just like CAPD. Most APD users keep extra dialysate bags on hand for exactly this reason. Some cyclers have battery backups, but they’re not reliable for full cycles. Always have a backup plan and know your emergency steps.
Which method has fewer infections?
APD has a lower rate of peritonitis-about 0.52 episodes per patient per year compared to 0.68 for CAPD. This is because APD uses a closed system with fewer manual connections. Each time you handle a bag in CAPD, you risk introducing bacteria. Even with perfect technique, the risk is higher. That’s why many doctors recommend APD for patients with a history of infections or those who struggle with sterile technique.
Can I travel with either type of dialysis?
Yes, both are travel-friendly, but differently. CAPD is easier-you just pack your dialysate bags and go. No machine, no power needed. APD requires you to ship or rent a cycler at your destination. Some companies offer travel kits with lightweight cyclers and pre-filled bags. But if you’re flying, you’ll need to coordinate with your provider ahead of time. CAPD gives you more spontaneity; APD requires more planning.
 Medications
Medications