Levothyroxine-PPI Dose Adjustment Calculator
Based on clinical research showing that patients taking both levothyroxine and PPIs often need dose adjustments to maintain proper thyroid function.
Results will appear here after calculation
If you’re taking levothyroxine for hypothyroidism and also use a proton pump inhibitor (PPI) like omeprazole or pantoprazole for heartburn, you might be unaware that these two medications are working against each other. It’s not a myth or a rumor - it’s a well-documented, clinically significant interaction that can leave you feeling tired, gaining weight, or struggling to get your thyroid levels right - even if you’re taking your pills exactly as prescribed.
Why Levothyroxine Needs Acid
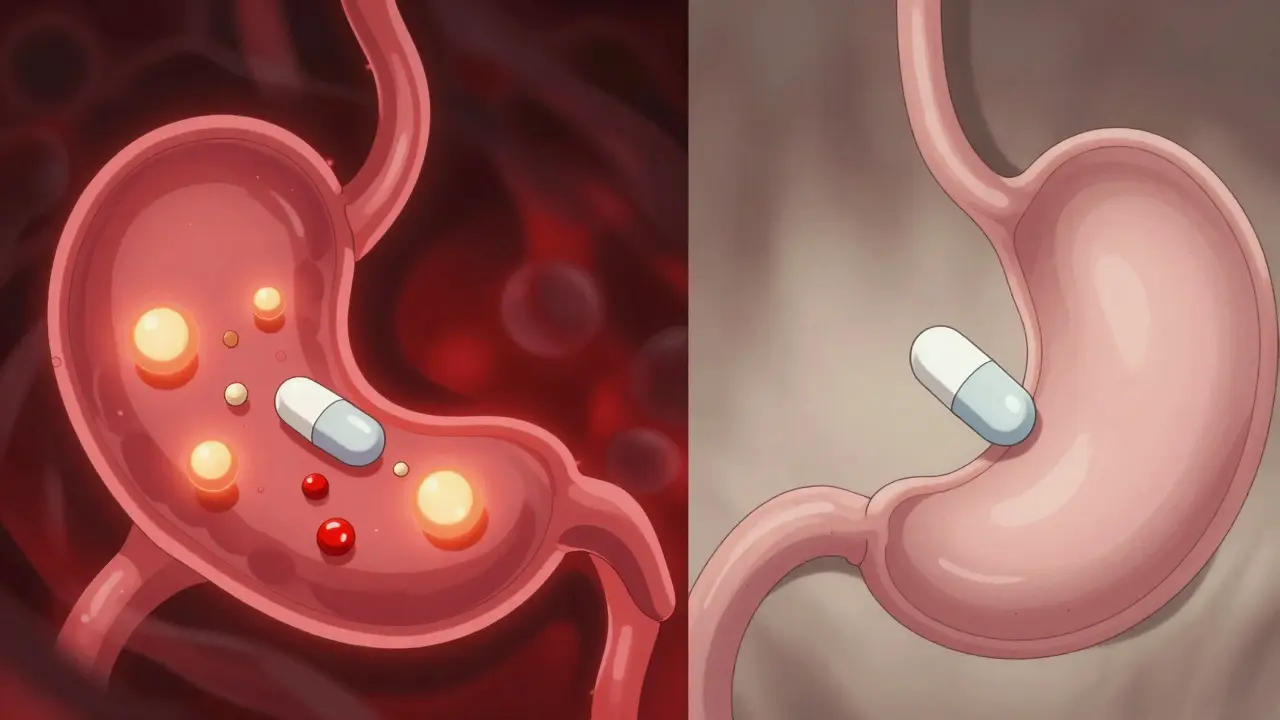
Levothyroxine isn’t like most pills. It doesn’t just dissolve in your stomach and get absorbed. It needs an acidic environment to break down properly. Your stomach normally has a pH between 1 and 2 - that’s as acidic as vinegar. This acidity is what allows levothyroxine tablets to dissolve and be absorbed into your bloodstream. Without it, the pill can pass through your system mostly intact, and your body never gets the full dose.
That’s where proton pump inhibitors come in. PPIs like omeprazole, esomeprazole, and pantoprazole are designed to shut down acid production. They target the proton pumps in your stomach lining - the very cells that make acid. After just a few days of use, your stomach pH can rise to 4 or 6. That’s not just less acidic - it’s nearly neutral. And that’s enough to block levothyroxine absorption.
The Evidence: TSH Levels Don’t Lie
A 2021 systematic review in the Journal of General Internal Medicine looked at seven studies involving thousands of patients. The results were clear: when people took levothyroxine and a PPI together, their TSH levels went up. Higher TSH means your thyroid isn’t getting enough hormone. Your body is screaming for more.
One 2023 study published in PubMed followed patients on 40 mg of pantoprazole daily for six weeks. All of them were previously stable on levothyroxine. After just six weeks, their TSH jumped - even when they took the PPI at night, hours after their thyroid pill. That’s the kicker: timing doesn’t fix it. PPIs suppress acid for up to 72 hours. Taking them 4 hours apart won’t help because the acid is still gone.
Who’s Affected? The Numbers Don’t Lie
About 20 million Americans take levothyroxine. Around 18% of them - nearly 3.6 million people - also take a PPI. That’s a massive overlap. And according to data from the Mayo Clinic Proceedings, about 15 to 20% of these patients need a higher dose of levothyroxine just to stay in range. On average, that’s an increase of 12.5 to 25 mcg per day. That’s not a small tweak. It’s enough to push someone from 75 mcg to 100 mcg - a jump that can take weeks to stabilize.
Real-world data from Reddit’s r/Hashimotos community backs this up. In a 2023 analysis of 147 posts, 68% of people reported needing a higher levothyroxine dose after starting a PPI. The most common complaints? Fatigue (72%) and unexplained weight gain (58%). These aren’t side effects of the PPI. They’re signs your thyroid medication isn’t working.

What Can You Do? Practical Solutions
There are three real options - not just "take it at a different time" - because that doesn’t work.
- Switch to liquid levothyroxine - Tirosint-SOL is a brand that uses glycerin instead of fillers that need acid to dissolve. A 2019 study in the Journal of Clinical Endocrinology & Metabolism confirmed it’s absorbed just fine even with PPIs. The catch? It costs $350 a month. Generic tablets are $15-$25. That’s a huge difference.
- Switch from PPIs to H2 blockers - Famotidine (Pepcid) is the most studied alternative. A 2018 study in Pharmacotherapy found no significant change in TSH when taken with levothyroxine. H2 blockers don’t shut down acid production as completely as PPIs. They’re weaker, but they’re safer for thyroid patients. If you only need occasional heartburn relief, this might be the best move.
- Monitor and adjust your dose - If you’re stuck on a PPI (say, because you have GERD or ulcers), don’t panic. Get your TSH checked before starting the PPI. Then test again at 6 to 8 weeks. If your TSH is up, your doctor can increase your levothyroxine by 12.5-25 mcg. Most people stabilize within 12 weeks, according to Cleveland Clinic data.
What About Short-Term Use?
If you’re only taking a PPI for a week or two - say, after a bad food reaction or while on antibiotics - you probably don’t need to worry. Dr. Elizabeth Pearce, an endocrinologist at Boston University, says short-term use (under 4 weeks) rarely causes meaningful absorption issues. But if you’re on a PPI for 3 months or longer? That’s when the risk spikes. And that’s when you need to act.
The Future: New Formulations on the Horizon
Drug makers are paying attention. The FDA issued draft guidance in 2023 specifically calling out PPI-levothyroxine interactions. Researchers are testing new enteric-coated levothyroxine pills that bypass the stomach entirely and dissolve in the small intestine - where acid isn’t needed. Phase 3 trials are ongoing (NCT04892357).
There’s also talk about generic versions of Tirosint-SOL. But it’s not easy. The formulation is patented, and replicating it without the same absorption profile is tough, as noted in the Journal of Pharmaceutical Sciences. The patent expires in 2025 - which could mean more affordable options soon.
What to Do Right Now
If you’re on both levothyroxine and a PPI:
- Check your last TSH result. Is it above your target range?
- Ask your doctor if you’ve had a TSH test in the last 3 months.
- If you’ve been on a PPI for more than 3 months and haven’t had your dose adjusted - bring it up.
- Ask if you can switch to famotidine for heartburn.
- If you’re on a PPI long-term and your symptoms (fatigue, weight gain) haven’t improved - ask about Tirosint-SOL.
This isn’t about stopping your PPI. It’s about making sure your thyroid medication works. Millions of people are stuck in a cycle of feeling worse - not because their condition is getting worse, but because their meds are fighting each other.
You don’t have to live with that.
What If You’re Not on PPIs But Still Feel Off?
Levothyroxine absorption can be messed up by other things too:
- Calcium supplements (take them 4+ hours apart)
- Iron supplements (same rule)
- Soymilk and high-fiber foods (take levothyroxine on an empty stomach, 30-60 minutes before eating)
- Antacids with aluminum or magnesium
But PPIs are the most common hidden culprit - especially in people over 50, who are more likely to have both hypothyroidism and acid reflux.
Can I just take my levothyroxine and PPI at different times of day?
No. Even if you take levothyroxine in the morning and your PPI at night, the acid suppression lasts for days. PPIs don’t wear off after a few hours. Studies show TSH levels still rise regardless of timing. The problem isn’t when you take them - it’s that the PPI shuts off acid production for up to 72 hours.
Is generic levothyroxine less affected than brand names?
No. All tablet forms of levothyroxine - whether it’s Synthroid, Levoxyl, or generic - rely on stomach acid to dissolve. The active ingredient is the same. The fillers may differ slightly, but none of them bypass the need for acidity. Only liquid formulations like Tirosint-SOL are designed to work without acid.
Can I stop my PPI if I’m feeling better?
Don’t stop PPIs suddenly without talking to your doctor. They can cause rebound acid hypersecretion, making heartburn worse. If you want to get off a PPI, work with your provider to taper slowly. You might be able to switch to an H2 blocker like famotidine, which doesn’t interfere with levothyroxine.
How often should I get my TSH checked if I’m on both medications?
Get tested before starting the PPI, then again at 6 to 8 weeks after starting it. After that, check every 6 months if you’re stable. If your dose changes, test again in 6-8 weeks. Many patients need dose adjustments - but you won’t know unless you test.
Does this interaction happen with all PPIs?
Yes. All proton pump inhibitors - omeprazole, esomeprazole, pantoprazole, lansoprazole, dexlansoprazole - work the same way. They reduce stomach acid. That’s the mechanism. So they all interfere with levothyroxine absorption. There’s no "safe" PPI for thyroid patients.
 Medications
Medications
Madhav Malhotra
January 11, 2026 AT 18:26Wow, this is insane-I’ve been on levothyroxine for years and just started omeprazole last month for acid. No wonder I’ve been so tired! My doc never mentioned this. Time to switch to Pepcid, I guess. Thanks for the clarity!
Jennifer Littler
January 11, 2026 AT 19:32Based on the pharmacokinetic data from the 2021 JGIM meta-analysis and the 2023 PubMed cohort study, the pharmacodynamic interference between PPI-mediated gastric acid suppression and levothyroxine’s pH-dependent dissolution kinetics is statistically significant (p<0.001). The TSH elevation is not merely correlational-it’s mechanistically causal. The 12.5–25 mcg dose escalation observed in Mayo Clinic data aligns with the 3-log reduction in gastric acidity. Tirosint-SOL’s glycerin-based formulation circumvents this entirely, but cost-benefit analysis must be individualized. H2RAs like famotidine preserve sufficient basal acid secretion (pH ~3.5) to permit absorption without compromising GERD control. This isn’t anecdotal-it’s evidence-based endocrinology.
Jason Shriner
January 13, 2026 AT 17:21so… i take my thyroid pill like a good boy… and then i take my acid pill like a good boy… and my body just… gives up? like, what is this, a soap opera? ‘the silent war of the stomach pumps’? i’m not mad, just disappointed. also, why does my life feel like a bad episode of ‘Grey’s Anatomy’?
Alfred Schmidt
January 15, 2026 AT 07:01THIS IS WHY YOU’RE STILL TIRED. YOUR DOCTOR ISN’T LISTENING. I WAS ON 100 MCG FOR YEARS, FELT LIKE A ZOMBIE, THEN FOUND OUT I WAS ON PANTOPRAZOLE-SWITCHED TO FAMOTIDINE, INCREASED TO 125 MCG, AND SUDDENLY I COULD BREATHE AGAIN. WHY IS THIS NOT STANDARD EDUCATION? WHY DO WE HAVE TO GOOGLE THIS LIKE COWBOYS? MY TSH WAS 8.7. NOW IT’S 1.9. I’M NOT ‘FINE.’ I’M ALIVE AGAIN.
Vincent Clarizio
January 16, 2026 AT 05:24Let’s take a step back and consider the existential implications of this. We are, all of us, tiny vessels navigating a biochemical labyrinth designed by evolution to sustain life-yet we are forced to weaponize chemistry against ourselves just to survive modern life. We take pills to suppress acid because we eat too much processed food, then we take pills to replace hormones because our thyroid is slowly surrendering to the chaos. And then we wonder why we’re exhausted. It’s not just a drug interaction-it’s a metaphor for the entire modern human condition. We patch ourselves with chemicals, hoping the system holds, while the machine we built to serve us slowly turns against us. Tirosint-SOL isn’t a medication-it’s a cry for help from a broken system. And the price? $350 a month. That’s not capitalism. That’s a funeral.
Sam Davies
January 16, 2026 AT 23:05Oh, so now we’re doing pharmacokinetic triage? How quaint. I mean, I suppose if you’re not rich enough for Tirosint-SOL, you’re just supposed to… suffer? And switch to Pepcid? How very 1998. I mean, at least we’ve got a PubMed citation to justify our suffering. Bravo. I’ll be sipping my chamomile tea while my TSH climbs, like a proper Victorian invalid.
Christian Basel
January 17, 2026 AT 00:17TL;DR: PPIs ruin levothyroxine. Switch to Pepcid or pay $350. Done.
Alex Smith
January 17, 2026 AT 04:28Hey, I’m glad this got shared-this is exactly the kind of info that gets buried in medical journals while people suffer. I’m a nurse, and I’ve seen this happen so many times. One patient, 68, on 100mcg levothyroxine, started omeprazole for ‘indigestion’ after a big meal. TSH jumped from 2.1 to 7.8 in 8 weeks. No one connected the dots until she came to me. We switched her to famotidine, upped her dose by 12.5, and she cried because she could finally walk up the stairs without stopping. This isn’t just science-it’s human. If you’re on both, get tested. Seriously. You don’t have to feel like this.
Roshan Joy
January 18, 2026 AT 07:36Thanks for this! 🙏 I’m from India and we don’t talk about this much here. My mom is on levothyroxine and was on omeprazole for years-she’s been so tired. We’re going to her doctor next week to switch to famotidine. Also, I just realized I’ve been taking calcium supplements with breakfast… no wonder she’s not feeling better 😅