When a critical medication expires, it’s not just a paperwork issue-it’s a patient safety emergency. In hospitals, ICUs, and even some long-term care facilities, an expired drug like fentanyl, midazolam, or norepinephrine can mean the difference between life and death. But you can’t just grab the next similar-looking pill from the shelf. You need a system. A clear, evidence-based way to decide what to use instead. And if you’re working in a hospital without one, you’re already behind.
Why Expired Medications Are Different from Shortages
Most people think expired meds and drug shortages are the same thing. They’re not. A shortage means the drug isn’t being made or shipped. An expired medication means it was there, but time ran out. The key difference? Expired drugs are often still physically present-just unusable. That means you have to replace them fast, with no time to wait for new shipments. In the ICU, patients are on 5 to 10 medications at once. One expired sedative? That could trigger withdrawal. One expired vasopressor? Blood pressure crashes. And if you guess wrong? You could cause organ failure, seizures, or cardiac arrest. This isn’t theoretical. In 2024, a study of 10,000 ICU cases found that when replacement protocols weren’t followed, medication errors led to 18.7% higher mortality rates.The Three-Tier Replacement System (ASHP Standard)
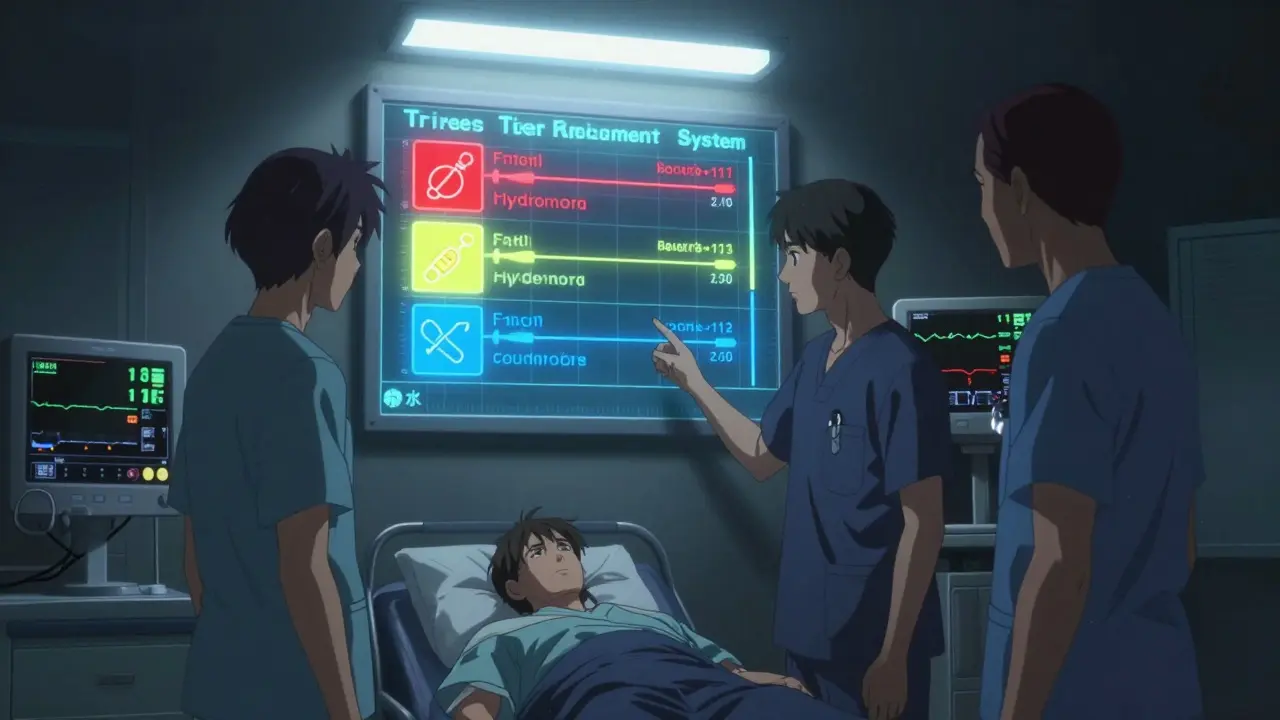
The American Society of Health-System Pharmacists (ASHP) has a proven framework for this exact problem. It’s called the three-tier system. It’s not a suggestion. It’s the gold standard used in 89% of academic medical centers. Here’s how it works:- 1st Line: Direct Therapeutic Equivalent - The exact same drug class, same mechanism, same dosing profile. For example, if your fentanyl infusion expires, hydromorphone is a 1st line replacement. It’s not identical, but it’s predictable. Dose conversion is well-documented.
- 2nd Line: Clinically Valid Alternative - A drug that works similarly but has different kinetics. Like switching from cisatracurium to rocuronium for neuromuscular blockade. You’ll need to adjust the dose, monitor longer, and watch for side effects.
- 3rd Line: Last Resort - Only if 1st and 2nd aren’t available. Maybe you’re forced to use vecuronium when rocuronium is out. It’s not ideal. It’s slower, harder to reverse. But it’s better than nothing.
How to Implement a Replacement Protocol in 7 Steps
You don’t need a big budget. You need structure. Here’s how to build one, even if you’re the only pharmacist on duty:- Validate the expiration - Don’t assume. Check the lot number, expiration date, and quantity. Was it stored correctly? Was it exposed to heat or light? Sometimes a drug looks expired but is still stable. The FDA’s 2025 draft guidance on shelf-life extension may soon make this easier, but for now, stick to the label.
- Count remaining stock - How much is left? Is it enough for one dose? Ten? If it’s 200 mL of something that lasts 48 hours, you have time. If it’s 10 mL? You’re in crisis mode.
- Identify affected patients - Who’s on this drug? How many? Are they ventilated? On dialysis? Kidney failure? This changes everything. A drug that’s safe for a healthy 30-year-old might kill someone with liver disease.
- Match to tiered alternatives - Pull up your ASHP protocol. Use the 1st line first. If you can’t get it, move to 2nd. Never skip tiers unless you’re out of options. Document why.
- Adjust doses - This is where mistakes happen. Fentanyl to hydromorphone isn’t 1:1. It’s roughly 1:10. Get it wrong, and you overdose or underdose. Always use a trusted conversion chart. Never rely on memory.
- Update the EHR and barcodes - If the system still shows fentanyl as active, someone will order it again. Change the inventory record. Flag the new drug in the order set. This step is often skipped-and it’s why errors repeat.
- Monitor and document - For the next 72 hours, track vital signs, sedation scores (RASS), and lab values. If the patient’s heart rate spikes or they start shivering, you might be seeing withdrawal. Log everything. This isn’t bureaucracy. It’s your legal protection.
Who Should Be on the Replacement Team?
This isn’t a pharmacist’s job alone. It’s a team sport. In high-performing hospitals, there’s a daily medication safety huddle-15 minutes, before rounds. Pharmacists, nurses, intensivists, and sometimes even respiratory therapists gather. They review: expired meds, upcoming expirations, pending orders, and any last-minute changes. Why does this work? Because nurses see the patient 12 times a day. They notice when someone’s restless. Pharmacists know the drugs. Doctors know the diagnosis. Together, they catch what no one person would see alone. In community hospitals? Only 42% have this. That’s why they have 3x more medication errors. If your hospital doesn’t have this, start it. Even if it’s just you and one nurse, meeting every morning. It changes outcomes.What Happens When You Don’t Have a Protocol?
In 2024, a Reddit post from an ICU nurse in rural Ohio went viral. Her hospital’s fentanyl expired. No pharmacist on site. No written guidelines. The team tried switching to morphine. Then to tramadol. Then to acetaminophen. The patient went into withdrawal. Had a seizure. Ended up in the ER again 11 days later. That’s not rare. The National Critical Care Survey found that hospitals without formal replacement protocols had 32% more medication-related readmissions. And those readmissions cost an average of $11,200 per patient. The worst part? Many of these errors are preventable. You don’t need AI. You don’t need a million-dollar system. You need a printed sheet with the three-tier list taped to the pharmacy counter.Technology Can Help-But It’s Not a Fix
Some hospitals use automated systems that alert them 30 days before a drug expires. Others use barcode scanning to block expired meds from being dispensed. AI tools are now being tested that analyze 147 patient factors-like kidney function, age, and current sedation level-to recommend the best replacement. But here’s the truth: technology doesn’t replace judgment. It supports it. A 2025 study at CU Anschutz found that AI-recommended replacements matched expert pharmacists 94.7% of the time. But when the AI was used without a pharmacist present? Errors doubled. Why? Because the AI didn’t know the patient’s history. It didn’t know the nurse had already seen withdrawal signs. It didn’t know the family had refused certain drugs. So use tech. But never trust it alone.
The Real Barrier: Lack of Pharmacists
The biggest reason hospitals struggle with expired meds isn’t money. It’s people. The American Association of Colleges of Pharmacy predicts a shortage of 112,000 pharmacists by 2027. Community hospitals already can’t afford full-time critical care pharmacists. So they rely on part-timers or none at all. That’s why 68.4% of community hospitals report inadequate medication management resources. And why the gap between academic centers (87% have protocols) and community hospitals (42%) keeps growing. If you’re in a small hospital, here’s what you can do:- Partner with a nearby academic center. Ask for their protocol. Most will share it.
- Use free ASHP resources. Their Drug Shortages Resource Center has downloadable checklists.
- Train your nurses. Teach them how to spot signs of withdrawal or overdose. They’re your eyes on the ground.
What’s Changing in 2026?
The ASHP is updating its guidelines this year. The new version will include specific protocols for expired medications-not just shortages. That’s huge. It means this won’t be an afterthought anymore. The FDA is also testing new expiration dating rules. Some drugs might now last longer than printed on the label. But until then, assume the date is final. And more hospitals are starting to tie reimbursement to medication safety. If your hospital has more than 15% of patients readmitted due to medication errors, CMS cuts your payments. That’s forcing change.Final Rule: Never Guess. Always Check.
There’s no shortcut. No magic pill. Just discipline. If a drug expires:- Don’t swap it with something that looks similar.
- Don’t use what’s left in the vial “just in case.”
- Don’t wait for the pharmacist to show up.
- Find your protocol.
- Know your tiers.
- Adjust the dose.
- Monitor like your patient’s life depends on it-because it does.
 Medications
Medications
Rachidi Toupé GAGNON
February 10, 2026 AT 17:25Bro this is the kind of post that makes me wanna hug a pharmacist 😭
Expired fentanyl? Nah, we got hydromorphone on deck like a boss. ASHP protocol? Printed, laminated, taped to the med cart.
One less nightmare in the ICU. You just saved someone’s life today, even if they don’t know it.
Pat Mun
February 12, 2026 AT 15:38I work in a 25-bed rural hospital with one part-time pharmacist who shows up Tuesdays and Thursdays.
Our protocol? A Google Doc someone made in 2019 that says ‘use what’s available’.
Yesterday, we ran out of norepinephrine. The nurse grabbed phenylephrine because it was ‘the red one’. Patient’s BP spiked to 220/110. We had to call the regional hospital for help.
It’s not that we don’t care. It’s that no one ever gave us a real system. This post? It’s the first time I’ve felt seen.
Maybe we start with printing the ASHP tiers and taping them to the fridge. It’s better than nothing. And honestly? Better than what we’ve got.
Robert Petersen
February 13, 2026 AT 13:03Love this. Seriously.
Not every hospital has a $2M EHR or AI that predicts withdrawal before it happens.
But every hospital has a nurse who notices when a patient won’t stop shaking. Every hospital has a tech who knows which vial is which. Every hospital has someone who cares enough to ask, ‘Wait, what’s the replacement?’
You don’t need fancy tech. You need a checklist and the courage to use it.
Start tomorrow. Tape it to the wall. Train the night shift. Do it like your life depends on it-because someone else’s does.
Suzette Smith
February 13, 2026 AT 20:36Wait, so you’re saying we shouldn’t just use whatever’s closest in color and shape? Whoa. Mind blown.
Next you’ll tell me not to use expired insulin because it’s ‘still kinda yellow’.
Skilken Awe
February 15, 2026 AT 03:20ASHP? Oh please. That’s just Big Pharma’s way of locking hospitals into their overpriced generics.
Real doctors don’t need tiered protocols. They use clinical judgment.
And let’s be real-how many of these ‘evidence-based’ conversions were funded by drug reps?
Also, why is everyone so scared of morphine? It’s been around since 1804. Maybe we should go back to the basics instead of overcomplicating with ‘1st line, 2nd line’ nonsense.
Kristin Jarecki
February 15, 2026 AT 23:12Thank you for this meticulously structured, clinically grounded piece. The three-tier system is not merely a guideline-it is a non-negotiable standard of care, grounded in decades of pharmacokinetic research and post-marketing surveillance.
What troubles me most is not the absence of protocols, but the normalization of improvisation in high-acuity environments.
When a nurse is forced to choose between two unverified alternatives, the cognitive load is not merely a workload issue-it is a systemic failure of institutional preparedness.
I urge every healthcare administrator reading this to allocate budget-not for new software, but for printed, laminated, and regularly audited clinical decision aids.
And yes, the medication safety huddle must be institutionalized, not optional. It is the last line of defense against preventable harm.
Every life lost due to a substitution error is a failure of leadership, not of individual clinician judgment.
Stephon Devereux
February 16, 2026 AT 10:51This is the kind of clarity we need more of.
It’s not about being perfect. It’s about being prepared.
I’ve seen too many good nurses panic because they were never taught what to do when the vial says ‘expired’.
It’s not their fault. It’s the system’s.
But here’s the beautiful part: you don’t need a hospital-wide overhaul to fix this.
One person. One printed sheet. One morning huddle.
That’s all it takes to turn chaos into control.
Start small. Start today. And when someone asks why you’re doing it, just say: ‘Because last week, someone almost died because we didn’t.’
Autumn Frankart
February 17, 2026 AT 13:41Did you know the FDA’s ‘shelf-life extension’ program was originally created by the military to save money on battlefield meds?
Now they’re quietly rolling it out to civilian hospitals… but they’re not telling you.
And guess who’s pushing this? The same companies that make the drugs.
They know expired meds are a cash cow.
They want you to think ‘expiration date = dead drug’ so you buy more.
But I’ve seen vials of epinephrine from 2018 that still worked perfectly.
They’re lying to you. The whole system is rigged.
Don’t trust the label. Don’t trust ASHP. Don’t trust the ‘experts’. Trust your own eyes. And your own gut.
And if you’re still buying from big pharma? You’re part of the problem.
Craig Staszak
February 18, 2026 AT 21:54Good stuff. The three-tier system is gold. But here’s the thing no one says.
It doesn’t matter how perfect your protocol is if your pharmacy tech doesn’t read.
I worked at a hospital where we had the whole ASHP guide printed and laminated.
But the tech kept pulling fentanyl because ‘it looked right’.
He didn’t even check the label.
So we started putting a red sticker on every expired vial.
And we made the techs say the drug name out loud before they grabbed it.
Now? Zero errors in 18 months.
Sometimes the fix isn’t knowledge. It’s a sticker and a habit.
Sophia Nelson
February 20, 2026 AT 10:04Why are we even talking about this? It’s 2026. Why are we still using paper protocols?
Why not just let the AI decide? It’s 94% accurate.
And if the AI says ‘use vecuronium’ and the patient dies? Who’s liable? The pharmacist? The nurse? Or the hospital that didn’t invest in tech?
Stop pretending this is about ‘judgment’. It’s about liability.
And if you’re still using laminated sheets, you’re just delaying the inevitable.
andres az
February 20, 2026 AT 15:16ASHP? More like ASHP-Pharma LLC.
Look at their funding sources.
Every ‘evidence-based’ conversion table has a drug company logo in the footer.
Hydromorphone? Made by Purdue.
Rocuronium? AstraZeneca.
They’re not giving you guidelines-they’re giving you sales pitches disguised as science.
And you’re drinking the Kool-Aid.
Real solution? Go generic. Go old-school. Use what’s been proven for 50 years-not what’s marketed this quarter.
steve sunio
February 22, 2026 AT 05:29you dont need a protocol u just need common sense
if the drug is expired u dont use it
if u dont have the replacement u dont give it
simple
why is this so hard
because hospitals are run by people who think powerpoint slides save lives
we are not fixing the problem
we are just making it look like we are
and then we wonder why people die
Steve DESTIVELLE
February 23, 2026 AT 09:07the expiration date is a social construct
time is not linear
the molecule does not care about your calendar
when we label a drug expired we are not declaring its death
we are declaring our fear
our fear of uncertainty
our fear of responsibility
the real crisis is not the expired drug
it is the system that forces us to see expiration as failure
and in that failure we forget that healing is not a checklist
it is a relationship
between patient and practitioner
and sometimes
between a vial and a hand that still believes in healing
alex clo
February 24, 2026 AT 10:33Thank you for this comprehensive and well-referenced overview. The integration of the ASHP three-tier framework into institutional policy is not merely advisable-it is a necessary component of quality assurance and risk mitigation in critical care settings.
Furthermore, the emphasis on interdisciplinary collaboration through structured huddles aligns with current best practices in patient safety, as outlined by the Joint Commission’s 2025 standards on medication reconciliation.
I would recommend that all facilities, regardless of size, implement a quarterly audit of their replacement protocols, with documentation of compliance and staff competency assessments.
This is not an administrative burden-it is a core tenet of professional accountability.
Stephon Devereux
February 24, 2026 AT 19:46One thing I’ve learned working in three different hospitals: the best protocol in the world means nothing if no one knows it exists.
So here’s what I do now.
Every time a new nurse starts, I hand them a laminated card. One side has the three tiers. The other has a QR code linking to the ASHP cheat sheet.
Then I say: ‘If you’re ever scared, if you’re ever unsure, if you’re about to grab something that looks close… stop. Look at this card. Then ask someone. Not because you’re dumb. Because we’re all human.
And we don’t let humans guess when lives are on the line.’
It’s not glamorous. But it works.